
Wernicke-ACC-Informed Therapy (WAIT): A Neurodevelopmental Clinical Proposal for a Trauma-Informed Alternative to Applied Behavior Analysis

Abstract
Applied Behavior Analysis (ABA) remains the most widely implemented intervention for autistic individuals in the United States, yet growing evidence from autistic communities and trauma-informed research calls its compliance-based model into serious question. This paper introduces Wernicke-ACC-Informed Therapy (WAIT), a neurodevelopmentally grounded clinical proposal for a relational alternative to ABA. WAIT is built on the convergent roles of two key brain regions: Wernicke’s Area, which is responsible for language comprehension, pragmatic processing, and social meaning, and the Anterior Cingulate Cortex (ACC), which governs affective empathy, error detection, emotional co-regulation, and self-monitoring. Drawing on the author’s Functional Conflict Perspective (FCP) and Mirror Integration Theory (MIT), along with established neuroscience, the vagal-linguistic hypothesis, and the Double Empathy Problem, WAIT replaces external compliance training with internalized self-regulation, comprehension-based communication, and relational co-regulation. This paper outlines the neurological rationale for WAIT, contrasts it with ABA across key clinical dimensions, proposes implementation strategies, and identifies directions for future empirical research. Implications for autism therapy reform are discussed through a trauma-informed and neurodiversity-affirming lens.
Keywords: autism, ABA alternative, Wernicke’s Area, anterior cingulate cortex, trauma-informed therapy, pragmatic language, neurodiversity, self-regulation, Double Empathy Problem, vagal-linguistic hypothesis
1. Introduction
Autism Spectrum Disorder (ASD) is a biologically based neurodevelopmental condition characterized by differences in social communication, sensory processing, and behavioral flexibility. The dominant intervention model in the United States is Applied Behavior Analysis (ABA), a framework developed in the 1960s and rooted in operant conditioning principles: external reinforcement, discrete trial training, and behavioral compliance. While ABA has accumulated decades of institutional support, it has also generated significant controversy. Autistic adults, trauma researchers, and neurodiversity advocates have consistently reported that its compliance-based structure produces lasting psychological harm (Kupferstein, 2018; Sandoval-Norton & Shkedy, 2019).
At the same time, advances in cognitive neuroscience have shed new light on the specific neural architecture underlying autistic communication, social processing, and self-regulation. The distinct functional roles of Wernicke’s Area and the Anterior Cingulate Cortex (ACC) are now better understood than they were when ABA was first developed. These findings suggest that autistic individuals do not lack social capacity, but rather process social and linguistic information through qualitatively different, bottom-up neural pathways. Interventions that fail to account for this neurodevelopmental reality risk causing harm through mismatch rather than facilitating growth through genuine alignment.
This paper proposes Wernicke-ACC-Informed Therapy (WAIT) as a neurodevelopmentally grounded, trauma-informed alternative to ABA. WAIT is designed to strengthen the brain’s natural pathways for language comprehension, social meaning-making, and emotional self-regulation, without coercion, external compliance demands, or the suppression of autistic communication styles. The theoretical foundations of WAIT draw from two frameworks developed by the author: the Functional Conflict Perspective (FCP), which reframes conflict and difference as adaptive regulatory mechanisms rather than deficits; and Mirror Integration Theory (MIT), which holds that healing occurs when internal cognitive and emotional states are met with accurate external reflection rather than correction.
The paper proceeds as follows: Section 2 reviews the neuroscientific basis for WAIT. Section 3 presents the core principles and clinical application of the model. Section 4 contrasts WAIT with ABA across key dimensions. Section 5 outlines implementation and training considerations. Section 6 discusses limitations and future research directions. Section 7 concludes with implications for autism therapy reform.
2. Neuroscientific Basis for WAIT
2.1 Wernicke’s Area and Pragmatic Language Processing
Wernicke’s Area, located in the posterior superior temporal gyrus of the dominant hemisphere, has long been associated with language comprehension. Contemporary neuroscience has expanded this understanding considerably. Wernicke’s Area is now understood to play a central role in pragmatic language processing, which includes the ability to interpret social context, implied meaning, figurative speech, irony, and connotation (Geschwind, 1970; Hagoort, 2005). These are precisely the areas where many autistic individuals experience the greatest difficulty, not because the capacity is absent, but because the efficiency and pathway of pragmatic processing differs.
Research on autistic language processing suggests that the pragmatic functions of Wernicke’s Area are not absent but underconnected, particularly in relation to frontal executive systems that support rapid, top-down meaning inference (Just et al., 2004). This underconnectivity produces the characteristically bottom-up, detail-first processing style observed in autism: highly precise and pattern-sensitive, but requiring more explicit scaffolding in order to extract social and contextual meaning.
Importantly, Wernicke’s Area shows neuroplasticity. Its pragmatic reasoning networks can be strengthened through structured, relational, and contextually rich linguistic input (Kana et al., 2006). WAIT is designed to provide exactly this kind of input: recursive, meaning-oriented, and embedded in genuine social exchange rather than scripted behavioral compliance.
2.2 The Anterior Cingulate Cortex (ACC) and Affective Co-Regulation
The Anterior Cingulate Cortex (ACC) sits at a critical intersection between cognitive control and emotional processing. Research shows that the ACC activates both during a person’s own experiences of pain or distress and during observation of distress in others, making it a key substrate of affective empathy and relational attunement (Singer et al., 2004). The ACC is also responsible for error detection, conflict monitoring, and initiating adaptive behavioral adjustments, all of which are essential to self-monitoring and social learning (Botvinick et al., 2004).
In autistic individuals, ACC activation patterns during social and emotional processing tasks differ from neurotypical norms (Di Martino et al., 2009). These differences are better understood as divergent regulatory styles rather than deficits. The autistic ACC may respond more strongly to sensory and interoceptive input, and may need co-regulatory scaffolding from an attuned partner in order to integrate affective feedback effectively.
ABA’s use of planned ignoring, extinction procedures, and token economies actively disrupts the co-regulatory process that the ACC depends on. WAIT, by contrast, uses relational attunement as its primary mechanism. Therapist or caregiver responsiveness to the child’s internal state is what activates and trains ACC-mediated self-regulation.
2.3 The Vagal-Linguistic Hypothesis: Broca’s and Wernicke’s Areas in Nervous System Context
The vagus nerve is the primary regulator of the autonomic nervous system’s social engagement system, as described in Porges’ Polyvagal Theory (2011). It may also functionally overlap with the brain’s primary language regions, including both Wernicke’s and Broca’s Areas. This vagal-linguistic interface suggests that language acquisition, social-behavioral conditioning, and nervous system regulation are not independent processes. They are deeply interwoven developmental pathways.
In autistic individuals, early experiences of nervous system dysregulation, whether due to sensory overwhelm, relational misattunement, or trauma, may disrupt the normal developmental integration of vagal regulation with linguistic and social learning. The result is not a failure of language acquisition, but a fragmentation of the grounded, embodied, relationally embedded context in which pragmatic language and social cognition typically develop.
This hypothesis has real implications for therapy design. If pragmatic language is partially regulated through vagal pathways, then interventions that dysregulate the nervous system through demand, unpredictability, correction, and compliance pressure will inherently interfere with the very processes they are trying to strengthen. WAIT is built around maintaining a regulated, predictable, and relationally safe therapeutic environment, which is the kind of context in which vagal-linguistic integration can actually take place.
2.4 Theory of Mind, Bottom-Up Processing, and the Double Empathy Problem
Deficits in Theory of Mind (ToM), the capacity to infer and represent the mental states of others, have historically been central to clinical accounts of autism (Baron-Cohen et al., 1985). However, the Double Empathy Problem (Milton, 2012) reframes this narrative. Autistic individuals do not lack empathy or social awareness. Rather, they operate within a qualitatively different social cognition framework. Difficulties in social interaction arise not from autistic deficit but from a bidirectional mismatch between autistic and non-autistic social processing styles.
ToM, as typically measured, reflects hierarchical, top-down processing: inferring a global social narrative from fragments of behavioral cues. Autistic cognition, which is characterized by bottom-up, detail-oriented, pattern-based processing, requires a different kind of scaffolding for social learning. Specifically, it benefits from explicit, transparent, meaning-centered communication rather than assumed shared inference. WAIT is built on this understanding.
3. Core Principles of Wernicke-ACC-Informed Therapy (WAIT)
WAIT is organized around five core clinical principles, each grounded in the neurodevelopmental and relational framework described above.
Principle 1: Language as an Internal Guide for Self-Regulation
Rather than using external compliance training, WAIT strengthens internal speech and self-monitoring by activating Wernicke’s Area for meaning comprehension and the ACC for error detection and adaptive adjustment. The primary clinical tool is guided verbalization: supporting the child to name, interpret, and respond to their own internal states through language.
Example (ABA approach): “Touch your nose.” [Child complies.] “Good job!”
Example (WAIT approach): “I see you’re frustrated. Can you tell me what’s wrong?” / “I don’t like this.” / “You don’t like this. What would help?”
The WAIT interaction builds Wernicke-Area-mediated comprehension of internal states and ACC-mediated self-monitoring, while keeping the relational environment safe and predictable.
Principle 2: Emotional Co-Regulation Through Natural Language
The ACC regulates emotional tone and social adaptation. WAIT replaces ABA’s extinction procedures (ignoring distress until the child complies) with relational co-regulation: the therapist attunes to the child’s affective state, validates verbalization of distress, and works with the child collaboratively rather than waiting for compliance. This activates the ACC’s affective empathy functions and trains internal error-correction without shame or suppression.
Example: A child struggling with task frustration is guided to say “This is hard, I need a break,” rather than being ignored until they either comply or shut down.
Principle 3: Conflict Resolution and Meaning-Based Adaptation
Wernicke’s Area processes ambiguity and social meaning, while the ACC manages cognitive conflict. WAIT prioritizes comprehension-based problem-solving over scripted response training. The goal is to help children understand why social norms exist, not simply to have them memorize behavioral outputs.
Example (ABA): “Say ‘thank you’ when someone gives you something.” (rote script)
Example (WAIT): “How do we show someone that what they did mattered to us? What does it feel like when someone acknowledges your effort?”
Principle 4: Intrinsic Motivation Over Extrinsic Compliance
WAIT replaces the token economy and reward/punishment architecture of ABA with curiosity-driven, relational, and meaning-centered engagement. Learning is embedded in genuine social experience rather than contingency management. This approach fosters ACC-mediated intrinsic motivation and Wernicke-Area-mediated contextual understanding, which are more durable foundations for social learning than externally managed compliance.
Principle 5: Pragmatic Language Scaffolding Without Forced Normalization
Many autistic individuals process language literally and find the inferential and contextual dimensions of social communication difficult, since those functions are processed through Wernicke’s Area. WAIT provides scaffolding that makes implicit social meaning explicit, without pressuring conformity to neurotypical communication styles.
Example: Rather than demanding eye contact, the therapist says: “You don’t have to look at me, but can you listen to my words and tell me what you think?” This keeps relational engagement intact without triggering the nervous system dysregulation that forced eye contact produces.
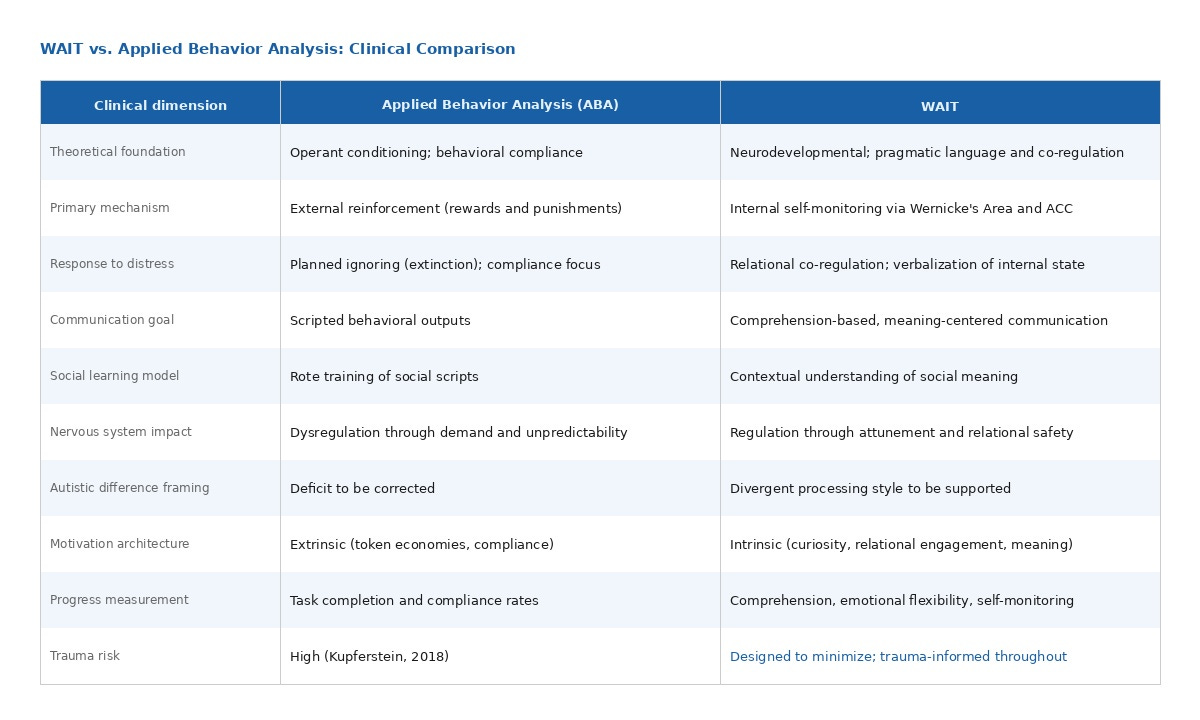
4. WAIT Compared to Applied Behavior Analysis
The following table contrasts WAIT and ABA across key clinical dimensions.
5. Implementation and Training Considerations
5.1 Therapist and Educator Training
WAIT requires a foundational shift in training orientation. Practitioners need to develop competency in neurodevelopmental frameworks of autism, pragmatic language processing, polyvagal-informed co-regulation, trauma-informed practice, and the Double Empathy Problem. Training should be developed in collaboration with autistic consultants and designed to move away from the compliance-based clinical assumptions that currently dominate the field.
5.2 Individualized Assessment and Profile-Guided Therapy
Each child’s linguistic, sensory, and regulatory profile needs to guide intervention design. WAIT rejects standardized compliance-based curricula in favor of individualized pathways that begin with the child’s current communication style, sensory environment, and relational context. Assessment tools should prioritize functional communication, emotional flexibility, and self-regulatory capacity over behavioral compliance benchmarks.
5.3 Family and Caregiver Integration
Co-regulation is most effective when it extends beyond the therapy room. WAIT includes structured caregiver coaching to support families in applying co-regulatory, meaning-centered communication in daily life. This approach reduces the neurological cost of context-switching between the therapeutic and home environments, and helps build relational safety as a consistent feature of the child’s daily experience.
5.4 School-Based Application
WAIT principles are designed to be scalable into school settings, replacing punitive behavioral management with restorative, co-regulatory models. Educators trained in WAIT can integrate guided verbalization, meaning-based social scaffolding, and sensory-informed environmental modifications into inclusive classroom practice.
5.5 Progress Measurement
Rather than tracking task completion and behavioral compliance, WAIT measures progress through growth in pragmatic language comprehension and use, increased emotional flexibility and self-regulatory capacity, reduction in distress-driven behavior (understood as communication rather than noncompliance), and qualitative improvement in relational engagement and sense of social belonging as reported by the child and family.
6. Limitations and Future Research Directions
WAIT is presented here as a clinical proposal grounded in established neuroscience and author-developed theoretical frameworks. It has not yet been subjected to randomized controlled trial research, and the author acknowledges this as a meaningful limitation. The framework’s neurological hypotheses, particularly the vagal-linguistic overlap and the neuroplasticity of pragmatic reasoning networks, need empirical testing with autistic populations.
Future research directions include the following. First, controlled studies comparing WAIT and ABA outcomes on measures of self-regulatory capacity, pragmatic language, and subjective well-being. Second, neuroimaging studies examining ACC and Wernicke’s Area activation patterns in response to WAIT-aligned versus compliance-based interventions. Third, participatory action research with autistic adults and youth as co-investigators to refine the WAIT model over time. Fourth, longitudinal studies on trauma outcomes associated with early compliance-based versus co-regulatory intervention models.
The author also recognizes the limitations of drawing on personal and familial experience with autism to support clinical claims. Lived experience is a legitimate and undervalued form of knowledge in neurodiversity research, but it needs to be examined alongside and tested against empirical evidence. The theoretical frameworks underpinning WAIT, namely FCP and MIT, are themselves in early stages of formal empirical development.
7. Conclusion
The dominance of Applied Behavior Analysis in autism intervention rests on a compliance-based model that was developed before contemporary understanding of autistic neurobiology, the Double Empathy Problem, and the neurological consequences of dysregulation and coercion. As neuroscience has advanced, the gap between what we know about how autistic brains work and what mainstream intervention asks of autistic children has grown wider, and the cost of that gap in trauma and lost potential is increasingly well-documented.
Wernicke-ACC-Informed Therapy (WAIT) offers a neurologically coherent, trauma-informed, and neurodiversity-affirming alternative. By targeting the brain’s natural pathways for meaning comprehension, affective co-regulation, and self-monitoring, WAIT holds that autistic individuals can develop robust social and communicative competence not through compliance, but through the same process that underlies all meaningful human development: safe, attuned, relational engagement with a world that is willing to meet them where they are.
This paper is offered as an invitation to the research community to examine, test, critique, and build upon the WAIT framework in genuine partnership with autistic people. Their knowledge of their own cognition and lived experience remains the most essential resource we have for autism therapy reform.
References
Baron-Cohen, S., Leslie, A. M., & Frith, U. (1985). Does the autistic child have a ‘theory of mind’? Cognition, 21(1), 37-46.
Botvinick, M. M., Cohen, J. D., & Carter, C. S. (2004). Conflict monitoring and anterior cingulate cortex: An update. Trends in Cognitive Sciences, 8(12), 539-546.
Di Martino, A., Ross, K., Uddin, L. Q., Sklar, A. B., Castellanos, F. X., & Milham, M. P. (2009). Functional brain correlates of social and nonsocial processes in autism spectrum disorders. Biological Psychiatry, 65(1), 63-74.
Geschwind, N. (1970). The organization of language and the brain. Science, 170(3961), 940-944.
Hagoort, P. (2005). On Broca, brain, and binding: A new framework. Trends in Cognitive Sciences, 9(9), 416-423.
Just, M. A., Cherkassky, V. L., Keller, T. A., & Minshew, N. J. (2004). Cortical activation and synchronization during sentence comprehension in high-functioning autism. Brain, 127(8), 1811-1821.
Kana, R. K., Keller, T. A., Cherkassky, V. L., Minshew, N. J., & Just, M. A. (2006). Sentence comprehension in autism: Thinking in pictures with decreased functional connectivity. Brain, 129(9), 2484-2493.
Kupferstein, H. (2018). Evidence of increased PTSD symptoms in autistics exposed to applied behavior analysis. Advances in Autism, 4(1), 19-29.
Milton, D. (2012). On the ontological status of autism: The ‘double empathy problem.’ Disability & Society, 27(6), 883-887.
Porges, S. W. (2011). The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation. W. W. Norton & Company.
Sandoval-Norton, A. H., & Shkedy, G. (2019). How much compliance is too much compliance: Is long-term ABA therapy abuse? Cogent Psychology, 6(1), 1644258.
Singer, T., Seymour, B., O’Doherty, J., Kaube, H., Dolan, R. J., & Frith, C. D. (2004). Empathy for pain involves the affective but not sensory components of pain. Science, 303(5661), 1157-1162.
Snow, I. S. (2025). Functional Conflict Perspective (FCP) and Mirror Integration Theory (MIT): Theoretical frameworks for relational healing and systemic transformation. SpiroLateral. https://spirolateral.org
Declaration of Generative AI and AI-Assisted Technologies in the Manuscript Preparation Process
During the preparation of this manuscript, the author used Claude (Anthropic, claude-sonnet-4-6) to assist with manuscript organization, academic language refinement, structural editing, and formatting of the clinical proposal. The author reviewed, revised, and takes full responsibility for all content, arguments, theoretical frameworks, and conclusions presented in this paper. The use of AI assistance did not replace the author’s intellectual contribution, clinical reasoning, or original theoretical development. All references were verified by the author. AI tools are not listed as authors or co-authors.