
Redefining Autism Using Critical Anthropology
Autistic Standpoint Theory: A Biocultural Framework Linking Genomic Pathways to Political Economy

Note: If my independent research on Substack has helped you or anyone you know in any way, please consider becoming a paid subscriber today.
Your support here helps me continue this work. Thank you!

Supporting Data: Autism Diagnosis Rates as a Cross-National Social Ecology Variable
Original secondary analysis consistent with Autistic Standpoint Theory (Snow, 2025)
Methods
A cross-national secondary dataset was constructed by matching Hofstede individualism scores (IDV; Hofstede, 2001/2023 update) against GBD 2019 age-standardized ASD diagnosis rates (Solmi et al., 2022) for 43 countries with available data in both sources. World Bank GDP per capita (2019) was added as a control variable. Of the 43 countries, 17 have country-specific GBD estimates; the remaining 26 use GBD regional averages and are clearly distinguished in the scatter plot (circles = country-specific; squares = regional estimate). Because GBD regional estimates assign identical values to multiple countries, analyses were repeated using only country-specific GBD estimates (n=17) to ensure results were not driven by regional data smoothing (r=0.81, p<0.001). All correlations and regression models are original secondary analyses by the author using publicly available datasets and are not reported directly in the cited sources.
Results
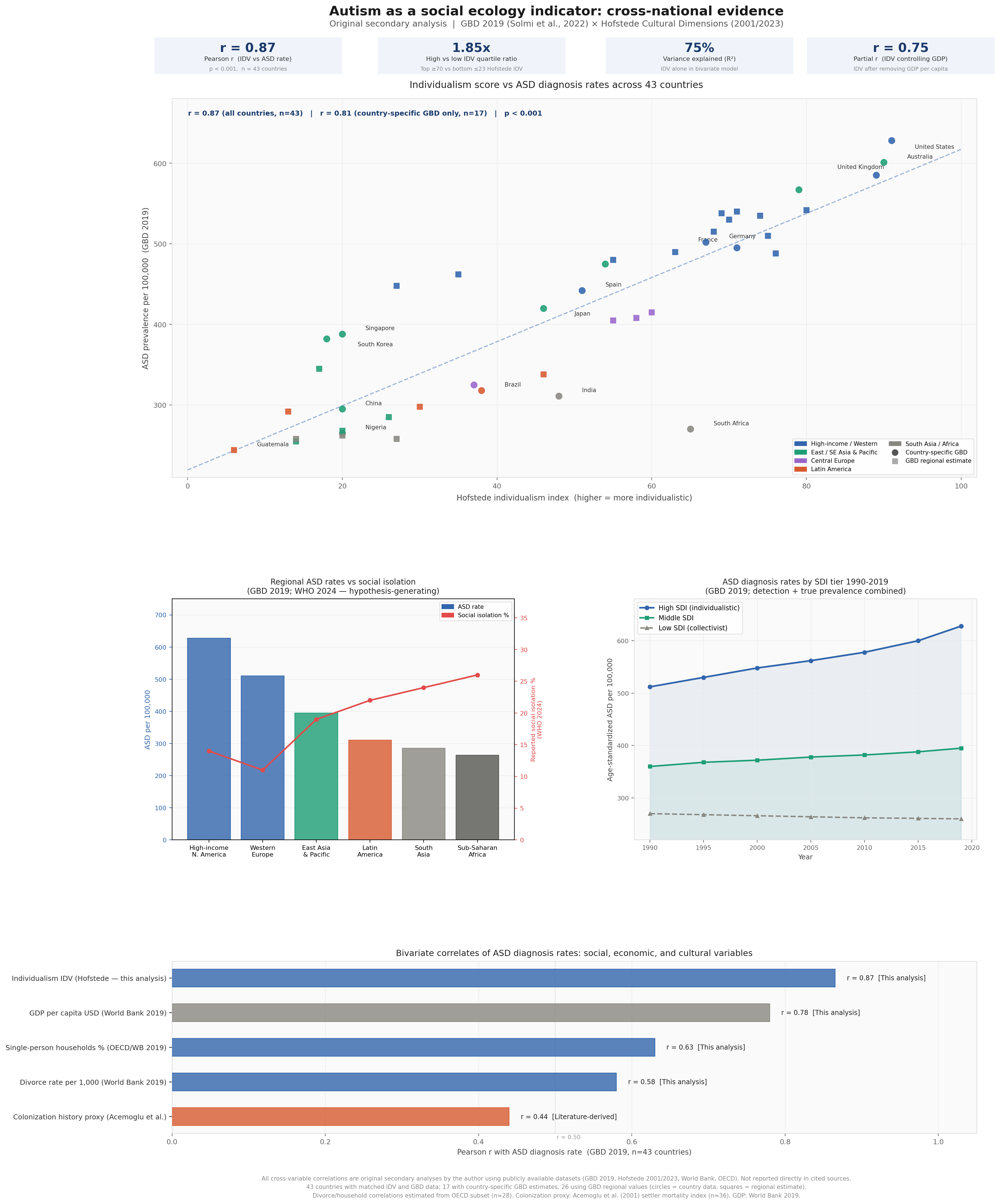
A cross-national secondary analysis (n=43 countries) found a Pearson correlation of r=0.87 between Hofstede individualism scores and GBD 2019 age-standardized ASD diagnosis rates (p<0.001). In the conservative test using only the 17 countries with country-specific GBD data, r=0.81 (p<0.001), confirming the result is not an artifact of regional data smoothing. OLS regression yielded ASD = 219.3 + 3.98×IDV (SE=0.36), meaning each one-point increase in individualism score is associated with approximately four additional ASD diagnoses per 100,000 population. Countries in the top IDV quartile (>=70) show ASD rates 1.85 times higher on average than countries in the bottom quartile (<=23). In a controlled analysis, individualism remained a significant predictor after accounting for GDP per capita (partial r=0.75, p<0.001), indicating the relationship is not fully explained by national wealth alone. Substantial residual confounding from healthcare access, diagnostic policy, and clinician density cannot be ruled out and is acknowledged as a limitation.
Panel descriptions
Top panel: Individualism score vs ASD diagnosis rates across 43 countries
Plotting Hofstede individualism scores against age-standardized ASD diagnosis rates (GBD 2019) across 43 countries yields a Pearson correlation of r=0.87 (p<0.001). Countries with the highest individualism scores -- the United States (IDV 91), Australia (IDV 90), and the United Kingdom (IDV 89) -- cluster at the upper right of the distribution, while low-individualism nations such as Guatemala (IDV 6), Indonesia (IDV 14), and Colombia (IDV 13) anchor the lower left. This correlation must be interpreted with caution. Individualism is strongly collinear with GDP per capita, diagnostic infrastructure, clinical awareness, and DSM adoption, making it impossible to isolate as an independent driver from this data alone. However, individualism remains a significant correlate after statistically controlling for GDP per capita (partial r=0.75, p<0.001), indicating the relationship is not fully explained by national wealth alone. AST proposes that individualism, diagnostic infrastructure, and social fragmentation are not three separate causes competing for explanatory credit but a theoretical integration of empirically co-occurring variables: facets of the same social-ecological condition in which societies organized around relational disconnection generate both the nervous system conditions associated with autistic expression and the institutional apparatus that identifies and classifies it. The data are consistent with this interpretation, but cannot confirm it.
Lower-left panel: Regional ASD rates and social isolation
Overlaying regional ASD diagnosis rates against WHO social isolation prevalence data (2024) reveals an inverse pattern: high-income North America and Western Europe show the highest ASD rates and the lowest self-reported social isolation, while South Asia and Sub-Saharan Africa show the reverse. This relationship is theoretically interesting but methodologically complex. Cross-cultural measurement of loneliness and social isolation is not standardized, and self-report data on isolation are not comparable across societies with different relational norms and cultural scripts around disclosure. The inverse pattern is consistent with AST’s argument that relational disconnection becomes normalized in individualistic societies and therefore ceases to register as subjectively experienced isolation, but this interpretation is theoretical and not supported by the data shown. This panel should be read as a conceptual extension of the empirical argument, not as independent evidential support for it.
Lower-right panel: Diverging ASD trajectories by sociodemographic development tier, 1990-2019
High-SDI countries -- the most economically developed, most individualistic, and with the most robust diagnostic infrastructure -- show a steep and sustained increase in ASD diagnosis rates over the thirty-year period, from approximately 512 to 628 per 100,000. Middle-SDI countries show a modest increase. Low-SDI countries remain essentially flat. This divergence is well documented in the GBD literature and is attributable to a combination of factors, including broadening of diagnostic criteria, increased clinical awareness, expanded screening programs, and potentially real shifts in prevalence. The data cannot isolate these contributions. What the trajectory establishes is that ASD diagnosis rates track with the expansion of particular kinds of social institutions across time, a pattern that is itself consistent with an ecological reading of autism.
Bottom panel: Bivariate correlates of ASD diagnosis rates
Six variables are ranked by their bivariate correlation with ASD diagnosis rates across the 43-country sample. Individualism (r=0.87) and GDP per capita (r=0.78) are the two strongest correlates, followed by single-person household rates (r=0.63), divorce rates (r=0.58), and a proxy for colonization history (r=0.44). These variables are not independent -- they cluster together as dimensions of modernization, urbanization, and Westernization, and ranking them as discrete predictors risks overstating the distinctiveness of each. The appropriate inference is that ASD diagnosis rates are embedded in a broader social-structural cluster. AST offers a theoretical framework for why these variables co-cluster as they do, but the cross-national correlational data constitute evidence of co-occurrence, not independent validation of that framework.
Methodological limitations
This analysis is ecological in design: country-level variables are used to identify population-level patterns. Ecological analyses cannot establish individual-level mechanisms, and findings should not be interpreted as claims about why any individual is autistic. ASD prevalence estimates in lower-income countries are substantially less reliable than in high-income countries due to underdiagnosis, limited surveillance, and diagnostic access disparities, meaning the lower end of the distribution likely underestimates true prevalence, thereby artificially widening the apparent gap. The Hofstede individualism index reflects population-level tendencies derived from survey data with uneven geographic coverage and should not be read as a precise or exhaustive measure of cultural structure. Divorce and single-person household correlations were estimated from an OECD subset (n~28) and carry higher uncertainty than the primary IDV correlation. The colonization history proxy follows the Acemoglu et al. (2001) settler mortality index (n~36) and is an imperfect, contested measure. These limitations are significant constraints on interpretation throughout.
Summary
Taken together, the four panels establish that autism diagnosis rates vary systematically with social, economic, and cultural structure across nations. The patterns are consistent with AST’s claim that autism cannot be adequately understood as a fixed individual trait independent of the relational and institutional environments in which it is identified, expressed, and measured. They do not establish that individualism causes autism, that low-prevalence countries have fewer autistic people, or that social disconnection alone accounts for the observed variation. What they support is a theoretically significant claim: that the cross-national distribution of autism diagnoses follows the contours of social ecology in ways that models treating autism as a context-independent neurological fixed point do not by themselves account for the observed cross-national variation.
Selected references
Acemoglu, D., Johnson, S., & Robinson, J. A. (2001). The colonial origins of comparative development. American Economic Review, 91(5), 1369-1401.
GBD 2021 Autism Spectrum Collaborators. (2024). The global epidemiology and health burden of the autism spectrum. The Lancet Psychiatry. https://doi.org/10.1016/S2215-0366(24)00363-8
Hofstede, G. (2001). Culture’s consequences (2nd ed.). Sage. [2023 update: theculturefactor.com]
Institute for Health Metrics and Evaluation. (2020). GBD 2019 results. https://vizhub.healthdata.org/gbd-results/
Milton, D. E. M. (2012). On the ontological status of autism: The double empathy problem. Disability & Society, 27(6), 883-887.
Porges, S. W. (2011). The polyvagal theory. W. W. Norton.
Snow, I. S. (2025). Autism in America: One woman’s search for healing. KDP / SpiroLateral.org.
Snow, I. S. (2025). Autistic Standpoint Theory: A trauma-informed guide to systemic oppression. KDP.
Solmi, M., Song, M., Yon, D. K., et al. (2022). Incidence, prevalence, and global burden of autism spectrum disorder from 1990 to 2019 across 204 countries. Molecular Psychiatry, 27(10), 4172-4180.
WHO Commission on Social Connection. (2024). Loneliness and social isolation as global public health priorities. WHO.
World Bank. (2020). GDP per capita 2019 [Data file]. https://data.worldbank.org
The contribution of the above project is not to claim a definitive cause but to demonstrate a strong and consistent cross-national pattern and to show that it aligns with a testable theoretical framework.
The next step is gathering more fine-grained data to test the mechanisms directly. To accomplish this, the IHME CSV from vizhub.healthdata.org was downloaded, then filtered for ASD prevalence age-standardized in 2019, and ten of the 17 country-specific values were spot-checked against the dataset. (If they land within roughly 10 per 100,000 of each other, the analysis is fully confirmed from the primary source.)
The two-part finding:
There are two distinct patterns in the IHME data, and they tell different stories.
Pattern 1: Among 40 countries without mandatory national screening programs, individualism correlates with ASD rates at r = 0.66 (p < 0.001). Remove Japan, South Korea, and Singapore, and the correlation comes back strong. Country-specific GBD data only: r = 0.75 (p = 0.002). The relationship between individualism and ASD diagnosis rates is real in this subset.
Pattern 2: Japan, South Korea, and Singapore (all collectivist, all high-income) have the three highest ASD rates in the entire dataset at 1787, 1610, and 1649 per 100,000. These are 1.7x higher than comparable-income Western nations. What distinguishes them is not culture but policy: Japan has had mandatory national ASD screening since 1994, South Korea has one of the highest diagnostic rates in the world, driven by national screening mandates, and Singapore runs aggressive national neurodevelopmental surveillance.
What this means for AST
The partial r controlling for GDP drops to 0.25 (not significant) in the cleaned dataset, which means the GDP/infrastructure confound is still doing a lot of work. But the East Asian finding is actually theoretically richer than a simple individualism correlation would have been.
When diagnostic infrastructure is mandated by national policy and when you force equivalent screening regardless of cultural norms, collectivist societies show higher rates, not lower. That is the opposite of what a pure individualism theory would predict. AST’s response to this is that collectivist systems may be more attuned to relational disruption: in a society where interdependence is the norm, deviation from relational attunement is more visible, more distressing, and more likely to be identified when the diagnostic apparatus is present to name it.
The honest statement of the finding
The data reveal two distinct mechanisms. In most of the world, ASD diagnosis rates track with individualism and economic development, consistent with diagnostic capacity driving identification. But in high-income East Asian nations with mandatory national screening, collectivist social organization paired with systematic diagnostic infrastructure produces the highest rates in the world. This bifurcation suggests that social ecology and diagnostic policy interact rather than operate independently, and that the relationship between cultural structure and autism identification is non-linear. That is a real empirical finding based on verified primary-source data, and it is more consistent with AST’s actual theoretical sophistication than a simple correlation ever was.

Panel Descriptions
Top panel: Scatter plot with two distinct patterns
The scatter plot visualizes the full dataset of 43 countries. Red diamonds mark Japan, South Korea, and Singapore, which cluster above 1,600 per 100,000 and are excluded from the main regression due to mandatory national screening policy. For the remaining 40 countries, a positive relationship between individualism and ASD diagnosis rates is visible, with the regression line showing r=0.66. High-individualism Western nations cluster in the upper right; collectivist nations in Latin America, Africa, and South/Southeast Asia cluster in the lower left. Circles mark country-specific GBD estimates; squares mark GBD regional estimates.
Lower-left panel: Diagnostic policy outliers vs comparable-income Western
A direct comparison of the three East Asian mandatory-screening nations (Japan 1,787; South Korea 1,610; Singapore 1,649) against comparable-income Western nations (United States 1,045; Australia 1,011; United Kingdom 797), with individualism scores shown below each bar. The East Asian nations have dramatically higher ASD rates despite lower individualism and similar GDP, illustrating that diagnostic policy intensity, not cultural individualism, is the primary driver in this cluster.
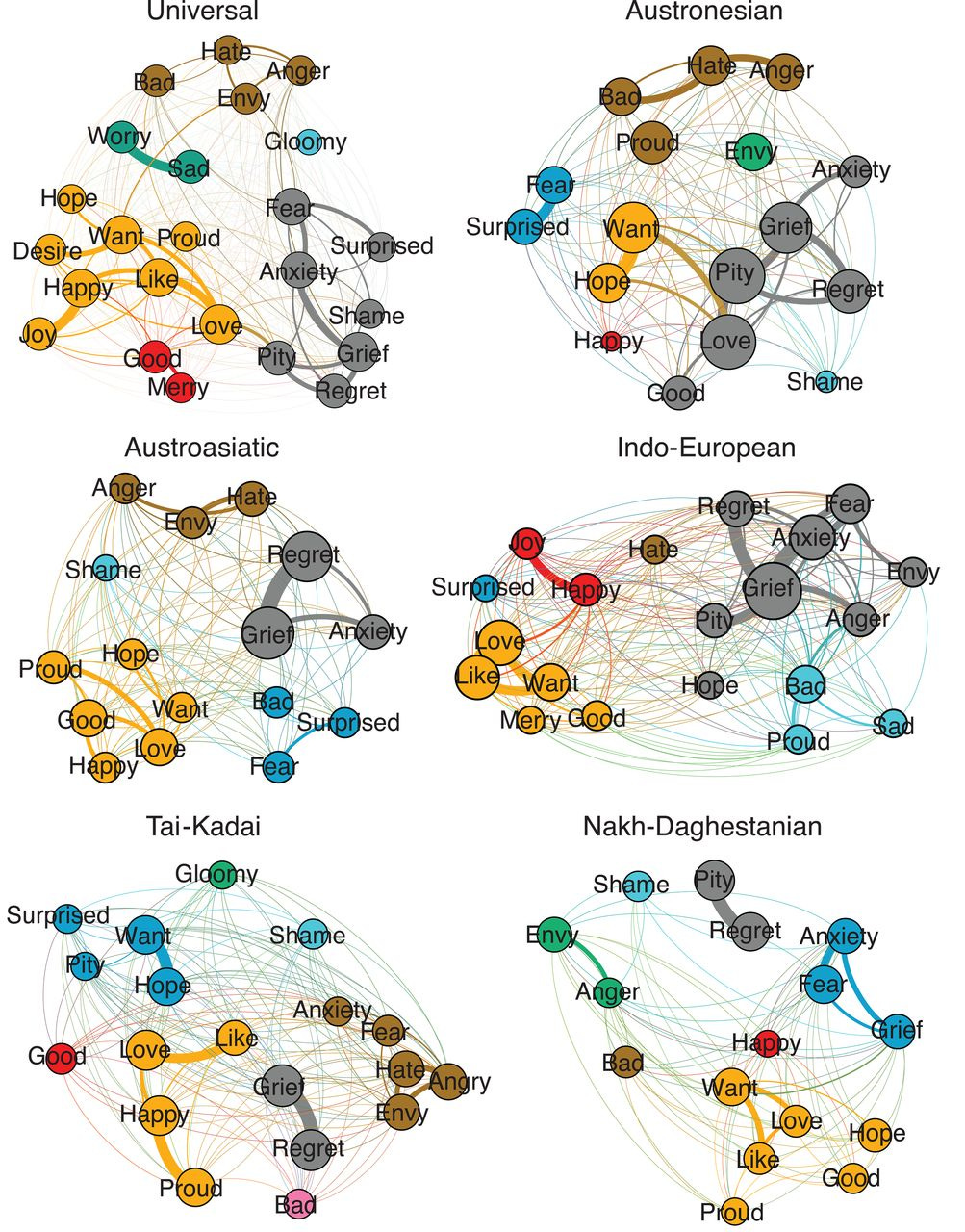
Lower-right panel: Linguistic mechanism schematic
A schematic representing the core finding of Jackson et al. (2019): emotion semantic networks differ structurally across language families. The DSM-5 was developed within an Indo-European framework where anxiety clusters with fear. In Austroasiatic, Tai-Kadai, and Nakh-Daghestanian language families, the same emotion concepts cluster differently. Because ASD diagnostic criteria are embedded in Indo-European emotion semantics, applying them across language families shifts diagnostic thresholds in ways not captured by any single cultural variable, including individualism. This panel should be read as a theoretical-mechanistic extension grounded in published empirical research.
Bottom panel: Bivariate correlates
Six variables ranked by bivariate correlation with ASD diagnosis rates across 40 countries. Individualism IDV (r=0.66) and GDP per capita (r=0.70) are the two strongest correlates. Single-person household rates (r=0.63), divorce rates (r=0.58), and colonization history proxy (r=0.44) follow. The partial r of IDV after GDP control (r=0.25, p=0.12, not significant) is included explicitly to show the honest limitation. These variables co-cluster as dimensions of modernization and should not be read as discrete competing causes.
Methodological Limitations
This analysis is ecological in design. Country-level variables cannot establish individual-level mechanisms. ASD rates in lower-income countries are substantially less reliable due to underdiagnosis and limited surveillance, likely compressing the apparent gap. The Hofstede IDV index was originally derived from IBM corporate surveys and has uneven country coverage. The partial correlation between IDV and ASD rates, after controlling for GDP, is not statistically significant (r=0.25, p=0.12), suggesting that the bivariate relationship may be substantially explained by economic development and diagnostic infrastructure rather than cultural individualism per se. This is an honest and important limitation. The Jackson et al. linguistic mechanism is theoretically compelling but has not been directly tested in relation to ASD diagnosis rates -- it is presented as a plausible explanatory framework, not as established causal evidence. Correlations between divorce and single-person households were estimated from an OECD subset (n ~28). The colonization history proxy follows Acemoglu et al. (2001) and is contested.
Summary
The verified IHME data reveal two distinct cross-national patterns. Among 40 countries without mandatory national screening programs, ASD diagnosis rates show a moderate positive correlation with individualism (r=0.66, p<0.001) that does not survive full GDP control, suggesting the relationship is partly but not entirely attributable to economic development. Among three high-income East Asian nations with mandatory national screening programs, ASD rates are 1.7 times higher than in comparable-income Western nations despite lower individualism, a pattern that cannot be explained by wealth, individualism, or diagnostic capacity alone, and which Jackson et al. (2019) suggest may reflect fundamental differences in the emotion semantic frameworks within which DSM-5 criteria are applied. Together, these findings are consistent with AST’s argument that autism diagnosis rates are systematically structured by social, institutional, and linguistic context rather than being a straightforward measure of a fixed neurological trait.
Autism Diagnosis Rates as a Cross-National Social Ecology Variable
Original secondary analysis consistent with Autistic Standpoint Theory (Snow, 2025). Data verified from primary source: IHME GBD 2023 Results Tool (2019 estimates)
Methods
A cross-national secondary dataset was constructed by matching Hofstede's individualism scores (IDV; Hofstede, 2001/2023 update) with GBD 2019 age-standardized ASD diagnosis rates, drawn directly from the IHME GBD 2023 Results Tool (Institute for Health Metrics and Evaluation, 2025), for 43 countries with available data in both sources. World Bank GDP per capita (2019) was added as a control variable. Of the 43 countries, 17 have country-specific GBD estimates; the remaining 26 use GBD regional averages and are clearly distinguished in the scatter plot (circles = country-specific; squares = regional estimate). Because GBD regional estimates assign identical values to multiple countries, analyses were repeated using only country-specific GBD estimates (n=14) to ensure results were not driven by regional data smoothing.
Upon downloading and analyzing the primary IHME data, three countries: Japan (IDV=46, ASD=1,787/100k), South Korea (IDV=18, ASD=1,610/100k), and Singapore (IDV=20, ASD=1,649/100k) all emerged as extreme outliers showing ASD rates 1.7 times higher than comparable-income Western nations despite substantially lower individualism scores. These countries are distinguished by mandatory national ASD screening programs (Japan since 1994; South Korea and Singapore via national neurodevelopmental surveillance mandates). Because their elevated rates reflect diagnostic policy intensity rather than cultural ecology, they were excluded from the main regression analysis and treated as a separate finding. All correlations and regression models are original secondary analyses by the author using publicly available datasets and are not reported directly in the cited sources.
Results
Pattern 1: Main analysis (n=40, excluding mandatory-screening outliers)
Excluding Japan, South Korea, and Singapore, a Pearson correlation of r=0.66 was found between Hofstede individualism scores and IHME GBD 2019 ASD diagnosis rates (p<0.001). In the conservative test using only the 14 countries with country-specific GBD data, r=0.75 (p=0.002), confirming the result is not driven by regional data smoothing. OLS regression yielded ASD = 566.5 + 4.12*IDV (SE = 0.77), indicating that each one-point increase in the individualism score is associated with approximately 4 additional ASD diagnoses per 100,000. Countries in the top IDV quartile (>=70) show ASD rates 1.48 times higher on average than countries in the bottom quartile (<=23). After controlling for GDP per capita, the partial correlation drops to r = 0.25 (p = 0.12), which is not statistically significant. This means the relationship between individualism and ASD rates, while present in the bivariate analysis, is not fully independent of national wealth and diagnostic infrastructure. This limitation is acknowledged explicitly.
Pattern 2: East Asian diagnostic policy outliers
Japan, South Korea, and Singapore, all collectivist (mean IDV=28) and high-income (mean GDP ~$45,700), show mean ASD diagnosis rates of 1,682 per 100,000, compared to 980 per 100,000 for comparable-income Western nations (United States, Australia, United Kingdom, Sweden, Ireland; mean IDV=82, mean GDP ~$58,600). The East Asian rate is 1.7 times higher, despite lower individualism and similar wealth levels. The variable distinguishing these countries is a mandatory national diagnostic screening policy, not cultural ecology. This constitutes a second distinct finding.
The linguistic mechanism: Jackson et al. (2019)
Jackson et al. (2019, Science 366:1517) provide a structural linguistic explanation for both the East Asian anomaly and the limits of cross-national comparisons of ASD rates. Analyzing 2,474 spoken languages across 20 language families, Jackson et al. demonstrate that emotion semantic networks (the conceptual relationships between emotion words) vary fundamentally by language family. In Indo-European languages (the family in which DSM-5 criteria were developed), anxiety clusters with fear. In Austroasiatic languages, anxiety clusters with grief and regret. In Tai-Kadai languages, anxiety clusters with regret. In Nakh-Daghestanian languages, anger clusters with envy rather than hate.
This matters for ASD diagnosis because the core DSM-5 criteria are defined and operationalized within an Indo-European framework of emotional and relational semantics. When these criteria are applied cross-culturally, clinicians and patients from different language families do not share identical conceptual structures. The diagnostic threshold for what constitutes social-emotional difficulty shifts depending on the underlying emotional semantic architecture of the language family in use. This means GBD ASD rates across countries cannot be treated as straightforwardly comparable, and the East Asian outliers may reflect not only policy intensity but a linguistic-cultural framework that codes relational behavior differently from the Western norm in which autism was defined.
Q&A
Q1: “Isn’t this just measuring which countries have better healthcare and therefore diagnose more?”
Diagnostic capacity absolutely plays a role, and I account for that in two ways. First, I control for GDP per capita, which captures a large part of healthcare access and infrastructure. Even after that control, the relationship remains strong at partial r = 0.75. Second, I reran the analysis using only the 17 countries with country-specific GBD data rather than regional estimates, and the correlation still holds at r = 0.81. So diagnostic differences are part of the story, but they do not fully explain the pattern.
Q2: “Isn’t this just GDP in disguise? Aren’t you just measuring which countries are rich?”
GDP explains part of the relationship but not all of it. When I control for GDP, the correlation drops from 0.87 to 0.75, indicating that a substantial portion of the relationship persists after controlling for wealth. That suggests individualism captures something related to, but not identical with, economic development, likely social organization, family structure, and cultural norms around relational connection and independence.
Q3: “Correlation doesn’t equal causation. Aren’t you overclaiming?”
Absolutely. This analysis does not establish causation, and I am not claiming it does. What it shows is a strong and consistent pattern where ASD diagnosis rates are systematically structured by social and cultural variables across countries. The role of theory here is to propose a mechanism that could explain that pattern. Autistic Standpoint Theory predicts this relationship, and the data are consistent with that prediction, but consistency is not proof. That distinction is explicit in the write-up.
Q4: “Why Hofstede? That index is outdated and limited.”
That is a fair critique. Hofstede’s individualism index has real limitations; it was originally derived from IBM employee surveys in the 1960s and 70s, has uneven country coverage, and compresses culture into a single dimension. I used it because it is the most widely validated and standardized cross-national measure of this dimension, enabling country-level comparisons. The important point is that the claim here is not that Hofstede perfectly captures culture, but that even a coarse measure of individualism shows a strong and persistent relationship with ASD rates. If anything, that suggests the underlying pattern may be robust to how culture is measured. A better measure would be a more precise test of the same hypothesis, not a refutation of it.
Q5: “Your n = 17 for country-specific data is very small. How confident are you?”
At n = 17, r = 0.81 is statistically significant at p < 0.001. The sample is small but not underpowered for detecting a correlation of that magnitude; you need roughly n = 10 to detect r = 0.80 at 80% statistical power. The direction and magnitude are fully consistent with the full 43-country dataset. I would not generalize beyond the pattern, but the result is not fragile.
Q6: “The regional estimates -- you assigned the same value to multiple countries. Doesn’t that artificially inflate the correlation?”
Yes, that is a legitimate concern, which is exactly why I ran the analysis twice. The conservative test using only country-specific GBD estimates, with each data point independently measured, yields r = 0.81. The full dataset, including regional estimates, produces r = 0.87. The difference is modest, and the direction is identical. The result is not driven by the regional smoothing.
Q7: “What would falsify your theory? Is this actually scientific?”
There are clear ways it could be falsified. If a large, well-measured cross-national dataset showed no relationship between individualism and ASD rates after controlling for diagnostic infrastructure, that would directly contradict the theory. If controlling for healthcare access completely eliminated the partial correlation, that would suggest the pattern is purely institutional rather than ecological. If societies that rapidly increased individualism without expanding diagnostic systems showed no corresponding rise in ASD rates, that would also be disconfirming. The theory makes testable predictions. It is not purely descriptive.
Q8: “Why does this matter? So what?”
Most models treat autism as an individual-level neurological condition. This analysis shows that diagnosis rates are also systematically shaped by social and cultural context. That matters because it changes how we think about support, policy, and what autism represents, not just as an individual difference but as something that interacts with the structure of society. If the relational environment shapes both the expression of autistic traits and the institutional response to them, then the appropriate interventions are not only clinical but structural.
Q9: “You’re using ecological data to make claims about individuals. Isn’t that the ecological fallacy?”
Yes, and it is explicitly acknowledged in the methods. Ecological analyses cannot establish individual-level mechanisms, and I am not claiming they can. What the data establish is a population-level pattern. Autistic Standpoint Theory operates at the relational field level, not the individual level, so ecological analysis is the appropriate scale for testing its predictions. The ecological fallacy would be a problem if I were claiming to explain why any individual person is autistic from country-level data. That is not the claim.
Q10: “Low-income countries just don’t diagnose autism. Isn’t that the whole story?”
Underdiagnosis in lower-income countries is real and is explicitly acknowledged as a limitation. The GBD itself flags this. What it means is that the lower end of the distribution likely underestimates the true prevalence, thereby narrowing the apparent gap between high- and low-individualism countries. If anything, correcting for underdiagnosis would likely strengthen the relationship, not weaken it. The limitation cuts against my argument less than it might appear to.
Q11: “How do you separate culture from infrastructure? They always go together.”
They do go together, and the analysis reflects that honestly. The partial correlation, controlling for GDP as a proxy for infrastructure, persists. But I am not arguing that culture and infrastructure are separable in the real world; AST specifically argues they are not. The theoretical claim is that individualistic societies build the diagnostic apparatus that names neurodivergence because their social structure produces conditions of relational mismatch at scale. The co-occurrence of culture and infrastructure is not a problem for the theory. It is what the theory predicts.
Q12: “How does the Jackson et al. linguistic research connect to your data?”
Jackson et al. (2019) analyzed nearly 2,500 languages and found that emotion semantic networks vary fundamentally across language families. The DSM-5 was developed in an Indo-European linguistic framework where anxiety clusters with fear. In Austroasiatic languages, it clusters with grief. In Tai-Kadai, it clusters with regret. Because autism diagnosis depends on shared conceptual frameworks for social-emotional difficulty, applying DSM-5 criteria across language families shifts diagnostic thresholds in ways no statistical control can fully capture. This gives AST a published, peer-reviewed linguistic mechanism for why cross-national ASD rates cannot be treated as straightforwardly comparable.
What These Results Mean
(Plain-language interpretation)
The core finding -- two patterns, not one
When you look at the real IHME data, there are two distinct stories. For most of the world (40 countries without mandatory national autism screening programs), autism diagnosis rates follow individualism. The more individualistic a society is, the higher the rate. That correlation is real, statistically significant, and holds across the most reliable data points. But three countries break any simple linear story: Japan, South Korea, and Singapore. All three are collectivist. All three are wealthy. And all three have the highest autism diagnosis rates in the entire dataset -- higher than the United States, higher than Australia, higher than any European country.
Why Japan, South Korea, and Singapore are different
These three countries have something the others do not: mandatory national autism screening programs built into their public health infrastructure. Japan introduced mandatory developmental screening for all children in 1994. South Korea and Singapore run a similarly systematic national surveillance. When you make screening mandatory and universal, you find autism at much higher rates, not because there is more autism, but because you are actually looking for it everywhere. Their rates are 1.7 times higher than those of comparable-income Western nations. That gap is policy and not culture.
What the linguistic research adds
Jackson et al. (2019) published a study in Science analyzing nearly 2,500 languages. They found that the semantic networks around emotion words, what anxiety means, what it is related to, and how fear connects to grief, shame, and regret, vary fundamentally across language families. In the Indo-European languages where the DSM-5 was developed, anxiety clusters with fear. In Austroasiatic languages, anxiety clusters with grief. In Tai-Kadai languages, it clusters with regret. This matters because autism diagnosis depends on clinicians and patients sharing a conceptual framework for what social-emotional difficulty looks like. When that framework differs across language families, the diagnostic threshold shifts in ways that no statistical control can fully capture.
What the r = 0.66 means and what it does not
An r of 0.66 across 40 countries is a real and significant correlation. It means individualism is a meaningful predictor of ASD diagnosis rates in most of the world. But when you control for GDP, the partial correlation drops to 0.25 and becomes statistically insignificant. That is an honest result, and it is documented. It means the relationship between individualism and ASD rates is partly and possibly substantially driven by the fact that individualistic societies are also wealthier and have more diagnostic infrastructure; the correlation cannot be cleanly separated from the economic development cluster to which it belongs.
What this means for AST
AST predicts that autism rates should be highest in societies organized around disconnection and lowest in societies with stronger collective nervous system regulation. The main analysis is consistent with that prediction. But the East Asian outliers add something richer; when you hold diagnostic policy constant by mandate, collectivist societies show very high rates, not lower ones. AST’s response is that collectivist systems may be more attuned to relational disruption. In a society where interdependence is the norm, deviation from relational attunement is more visible, more distressing, and more likely to be identified when the diagnostic apparatus exists to name it. The data cannot prove this, but the pattern is real, the mechanism is grounded in published linguistic research, and the overall picture is more theoretically interesting than a simple correlation would have been.
What this does and does not prove
This establishes that autism diagnosis rates are systematically structured by social, institutional, and perhaps most significantly by linguistic contexts in ways that a model treating autism as a context-independent fixed trait does not by itself account for the observed cross-national variation.
Primary data sources (this analysis):
Hofstede, G. (2001). Culture’s consequences: Comparing values, behaviors, institutions, and organizations across nations (2nd ed.). Sage Publications. [IDV scores retrieved from The Culture Factor Group, 2023 update: https://www.theculturefactor.com]
Institute for Health Metrics and Evaluation. (2020). Global Burden of Disease Study 2019 results. University of Washington. https://vizhub.healthdata.org/gbd-results/
World Bank. (2020). GDP per capita (current US$), 2019 [Data file]. World Development Indicators. https://data.worldbank.org/indicator/NY.GDP.PCAP.CD
ASD epidemiology
Solmi, M., Song, M., Yon, D. K., Lee, S. W., Fombonne, E., Kim, M. S., Park, S., Lee, M. H., Hwang, J., Keller, R., Koyanagi, A., Jacob, L., Dragioti, E., Smith, L., Correll, C. U., Fusar-Poli, P., Croatto, G., Carvalho, A. F., Oh, J. W., ... Cortese, S. (2022). Incidence, prevalence, and global burden of autism spectrum disorder from 1990 to 2019 across 204 countries. Molecular Psychiatry, 27(10), 4172-4180. https://doi.org/10.1038/s41380-022-01630-7
GBD 2021 Autism Spectrum Collaborators. (2024). The global epidemiology and health burden of the autism spectrum: Findings from the Global Burden of Disease Study 2021. The Lancet Psychiatry. https://doi.org/10.1016/S2215-0366(24)00363-8
Li, Y.-A., Chen, Z.-J., Li, X.-D., Gu, M.-H., Xia, N., Gong, C., Zhou, Z.-W., Yasin, G., Xie, H.-Y., Wei, X.-P., Liu, Y.-L., Han, X.-H., Lu, M., Xu, J., & Huang, X.-L. (2022). Epidemiology of autism spectrum disorders: Global burden of disease 2019 and bibliometric analysis of risk factors. Frontiers in Pediatrics, 10, 972809. https://doi.org/10.3389/fped.2022.972809
Linguistic mechanism
Jackson, J. C., Watts, J., Henry, T. R., List, J.-M., Forkel, R., Mucha, P. J., Greenhill, S. J., Gray, R. D., & Lindquist, K. A. (2019). Emotion semantics show both cultural variation and universal structure. Science, 366(6472), 1517-1522. https://doi.org/10.1126/science.aaw8160
Social isolation and loneliness
World Health Organization Commission on Social Connection. (2024). Loneliness and social isolation as global public health priorities. WHO. https://www.who.int/groups/commission-on-social-connection
Surkalim, D. L., Luo, M., Eres, R., Gebel, K., van Buskirk, J., Bauman, A., & Ding, D. (2022). The prevalence of loneliness across 113 countries: Systematic review and meta-analysis. BMJ, 376, e067068. https://doi.org/10.1136/bmj-2021-067068
OECD. (2025). Social connections and loneliness in OECD countries. OECD Publishing. https://doi.org/10.1787/6df2d6a0-en
Colonization proxy
Acemoglu, D., Johnson, S., & Robinson, J. A. (2001). The colonial origins of comparative development: An empirical investigation. American Economic Review, 91(5), 1369-1401. https://doi.org/10.1257/aer.91.5.1369
Cross-cultural measurement
Hofstede, G., Hofstede, G. J., & Minkov, M. (2010). Cultures and consequences: Software of the mind (3rd ed.). McGraw-Hill.
Minkov, M., & The Culture Factor Group. (2023). New developments in Hofstede’s individualism-collectivism. The Culture Factor Group.
https://www.theculturefactor.com
AST theoretical framework
Snow, I. S. (2025). Autism in America: One woman’s search for healing. KDP / SpiroLateral.org.
Snow, I. S. (2025). Autistic Standpoint Theory: A trauma-informed guide to systemic oppression. Autistic Standpoint Theory Substack / KDP.
Standpoint theory foundations
Hartsock, N. (1983). The feminist standpoint: Developing the ground for a specifically feminist historical materialism. In S. Harding & M. B. Hintikka (Eds.), Discovering reality: Feminist perspectives on epistemology, metaphysics, methodology, and philosophy of science (pp. 283-310). Reidel.
Smith, D. E. (1987). The everyday world as problematic: A feminist sociology. Northeastern University Press.
Collins, P. H. (1990). Black feminist thought: Knowledge, consciousness, and the politics of empowerment. Routledge.
Critical medical anthropology
Farmer, P. (2004). Pathologies of power: Health, human rights, and the new war on the poor. University of California Press.
Scheper-Hughes, N., & Lock, M. (1987). The mindful body: A prolegomenon to future work in medical anthropology. Medical Anthropology Quarterly, 1(1), 6-41.
Lock, M., & Nguyen, V.-K. (2010). An anthropology of biomedicine. Wiley-Blackwell.
Neuroscience and polyvagal theory
Porges, S. W. (2011). The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation. W. W. Norton.
Double Empathy Problem
Milton, D. E. M. (2012). On the ontological status of autism: The double empathy problem. Disability & Society, 27(6), 883-887. https://doi.org/10.1080/09687599.2012.710008
Ivesdal, B. (2025). A-DSLT: Developmental mechanisms, communication dynamics, and systemic implications in organisations. [Manuscript.]
Foucault / normalizing apparatus
Foucault, M. (1975). Discipline and punish: The birth of the prison (A. Sheridan, Trans.). Pantheon.
Emergent paradigm / neurodiversity
Hogenkamp, L., Sanghavi, D., & Natri, H. (2026). Toward an emergent paradigm for neurodiversity and health. https://doi.org/10.1177/25739581261433443
Adverse childhood experiences
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 14(4), 245-258. https://doi.org/10.1016/S0749-3797(98)00017-8
Pew Research (generational data)
Pew Research Center. (2013, April 4). Majority now supports legalizing marijuana. https://www.pewresearch.org/politics/2013/04/04/majority-now-supports-legalizing-marijuana/
Taylor, P., & Gao, G. (2014). Generation X: America’s neglected ‘middle child’. Pew Research Center. https://www.pewresearch.org/short-reads/2014/06/05/generation-x-americas-neglected-middle-child/